
For the first time since 2012, the American College of Cardiology (ACC) and American Heart Association (AHA) Guidelines for the Evaluation and Diagnosis of Chest Pain have been updated. The 2021 Guidelines now highlight use of Coronary CTA + FFRCT as a front-line pathway1, a decision that was supported by numerous clinical studies indicating that this pathway provides higher diagnostic accuracy compared to other non-invasive diagnostic tests2, provides long-term outcomes3 and is a “dominant strategy”.4
The newly updated ACC/AHA Guidelines reflect the growing support for a Coronary CTA + FFRCT pathway across the world–including in Europe (2019 ESC Guidelines), the UK (2016 NICE Guidelines) and Japan (2018 JCS Guidelines)–suggesting a revolutionary shift in the diagnosis and management of coronary artery disease (CAD) is underway.
Coronary CTA (CCTA) has been elevated to be the only Class I test with Level A evidence for use as a first-line tool to evaluate patients exhibiting symptoms of CAD: “it is effective for diagnosis of CAD, risk stratification, and guiding treatment decisions”. It is also appropriate after inconclusive functional tests, such as nuclear tests and stress echos, when considering revascularization strategies.
CCTA provides 98% negative predictive value and is a definitive test to help rule out the possibility of CAD.5

FFRCT is now included in the guidelines to support the further evaluation of patients with a coronary artery disease of uncertain physiologic significance. FFRCT provides actionable information that enables physicians to non-invasively diagnose “vessel-specific ischemia and guide decision-making regarding” revascularization in stenoses of 40-90%.
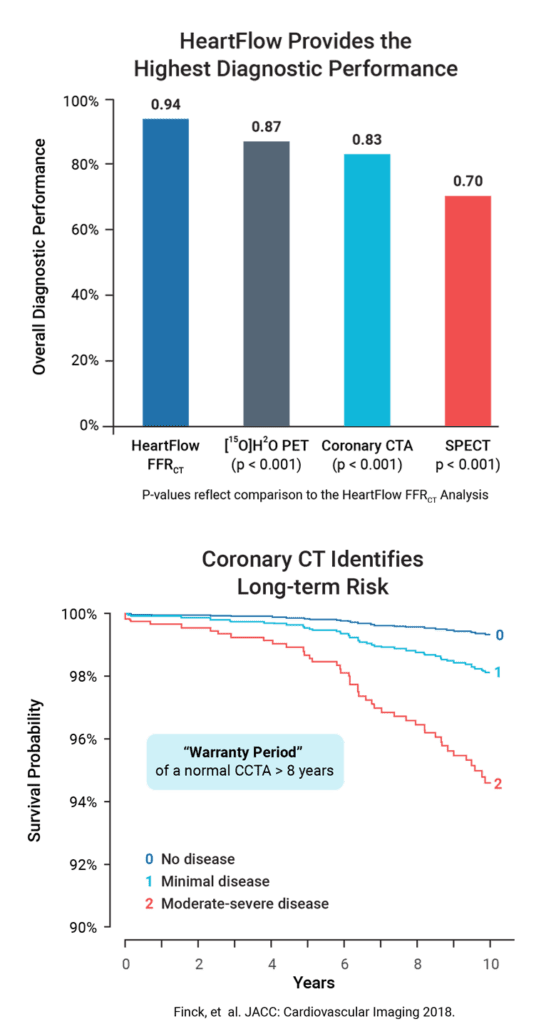
As the only commercially available FFRCT product, the HeartFlow FFRCT Analysis provides higher diagnostic performance and accuracy than other non-invasive tests.2
To date, more than 170,000 patients have benefited from a HeartFlow Analysis, but this is only a fraction of the 18+ million people living with coronary artery disease (CAD) in the US.6 Together, we can help take the stress out of the diagnosis and management of CAD and help revolutionize precision heart care.
Patients can stress less knowing that the most advanced technology available has been used to determine that either their CAD has been safely ruled out as a possible cause of their symptoms or that they are receiving the optimal treatment if CAD has been identified.
Physicians can stress less knowing that they have the clarity and confidence to precisely diagnose and treat their patients with CAD, benefiting from a single pathway that provides both anatomic and physiologic information in a simple-to-understand 3D model.
Hospital administrators can stress less knowing that their sites are delivering the best guideline-directed care, backed by major societies, payors, CMS and a growing coalition around the world all dedicated to addressing the most prevalent and deadly disease in the world.
The 2021 ACC/AHA Guidelines are built upon extensive evidence demonstrating the value of non-invasive cardiac testing. In particular, this evidence substantiates the long-term benefits of the CT+HeartFlow pathway, including:
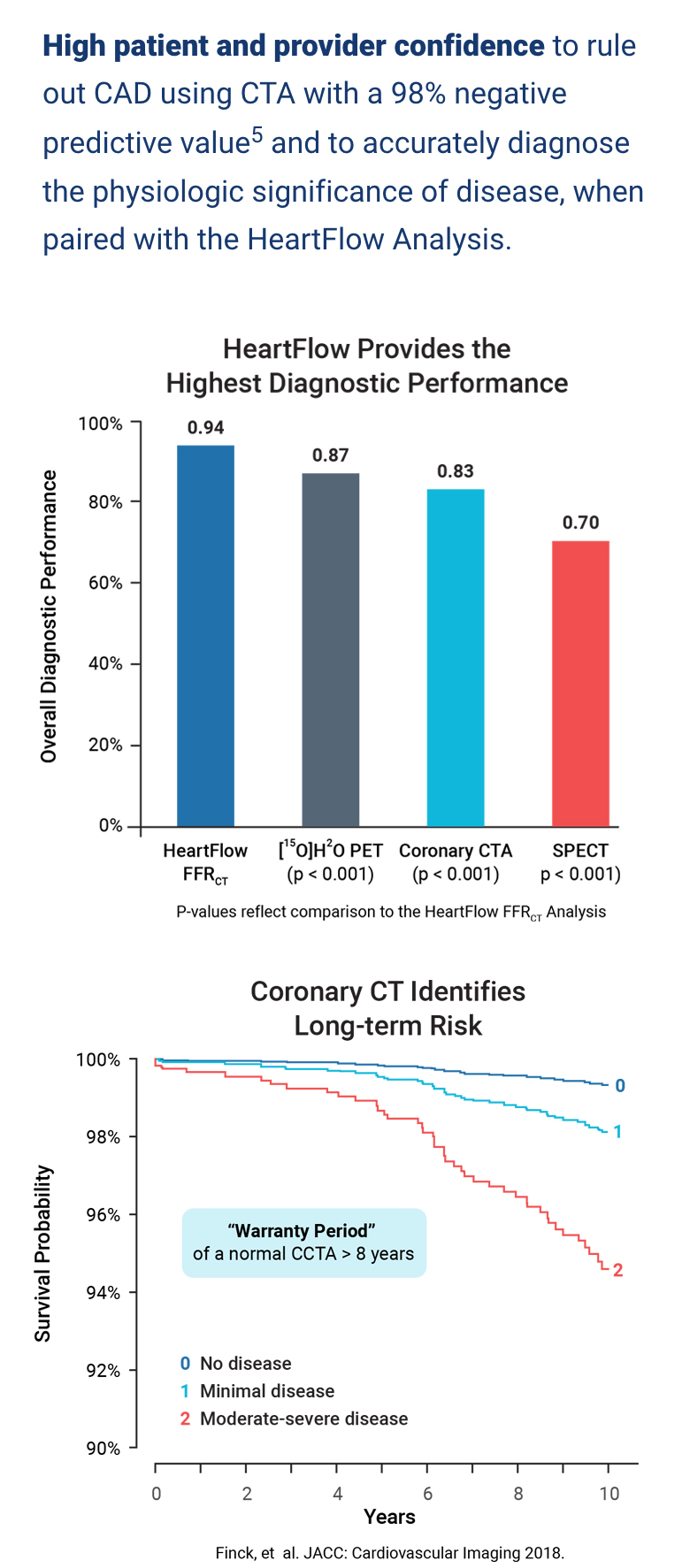
High patient and provider confidence to rule out CAD using CTA with a 98% negative predictive value5 and to accurately diagnose the physiologic significance of disease, when paired with the HeartFlow Analysis.
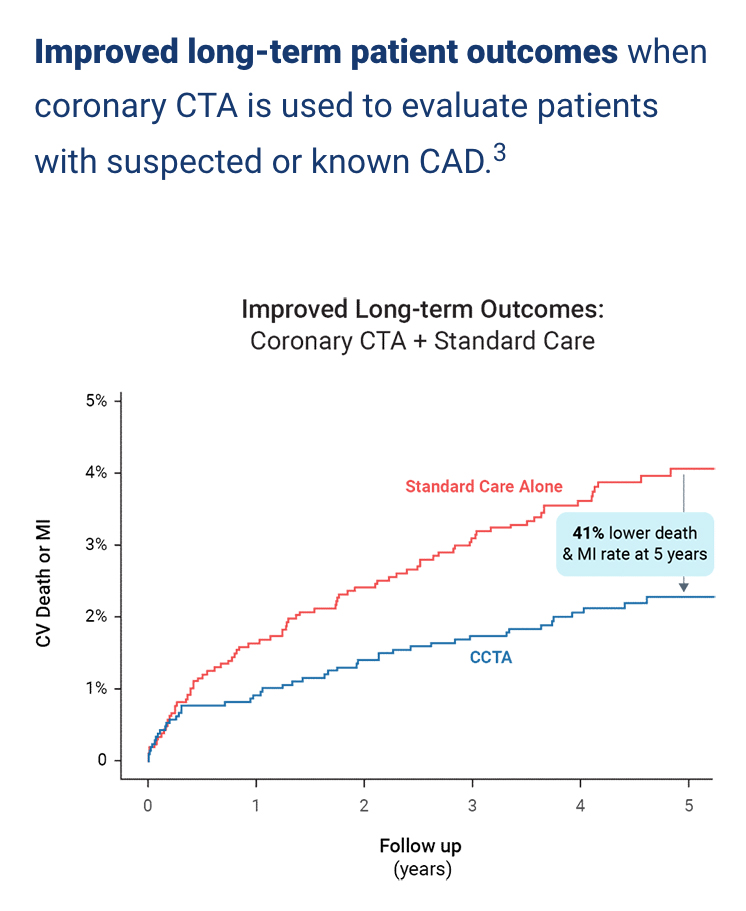
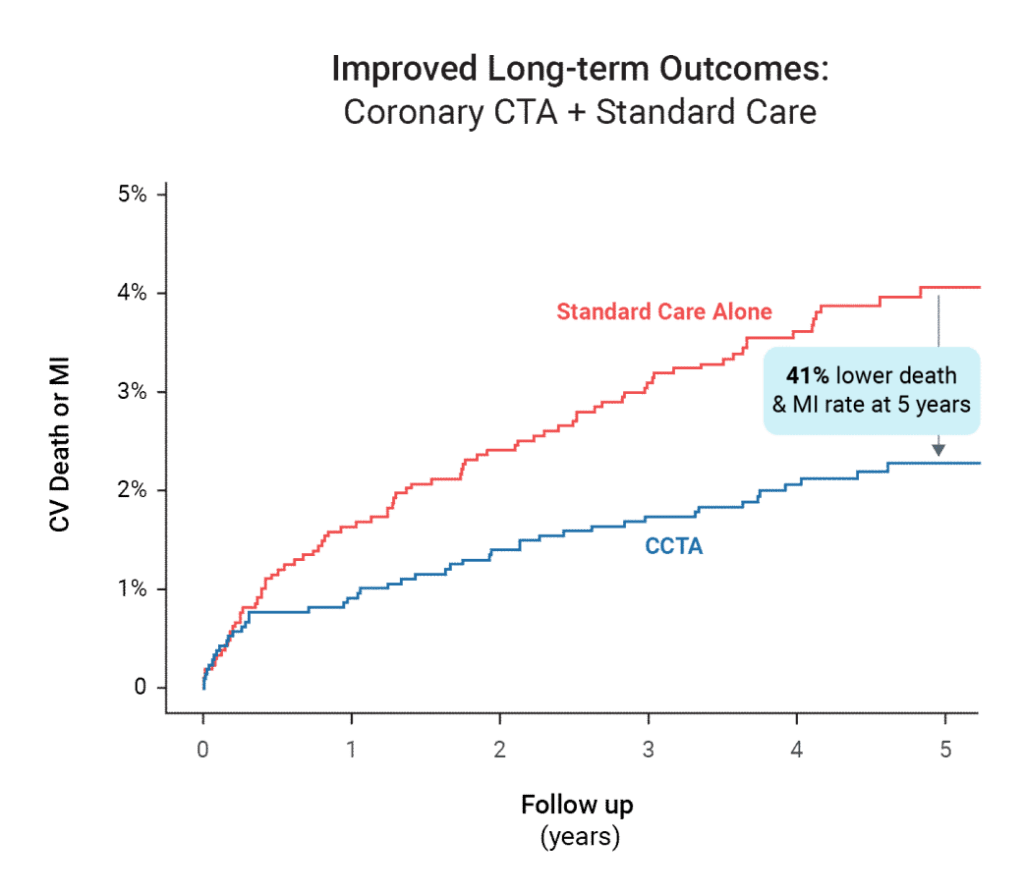
Improved long-term patient outcomes when coronary CTA is used to evaluate patients with suspected or known CAD.3
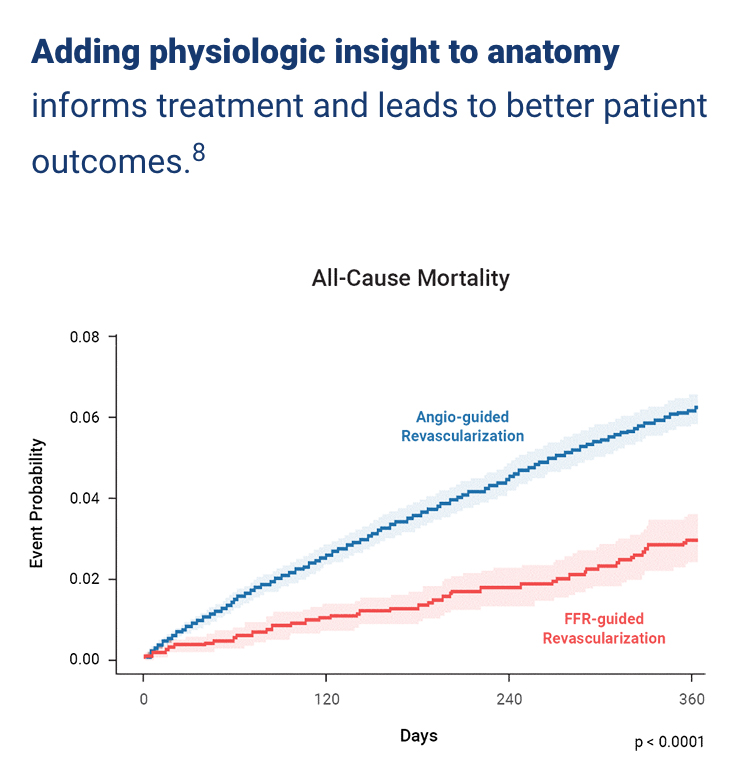
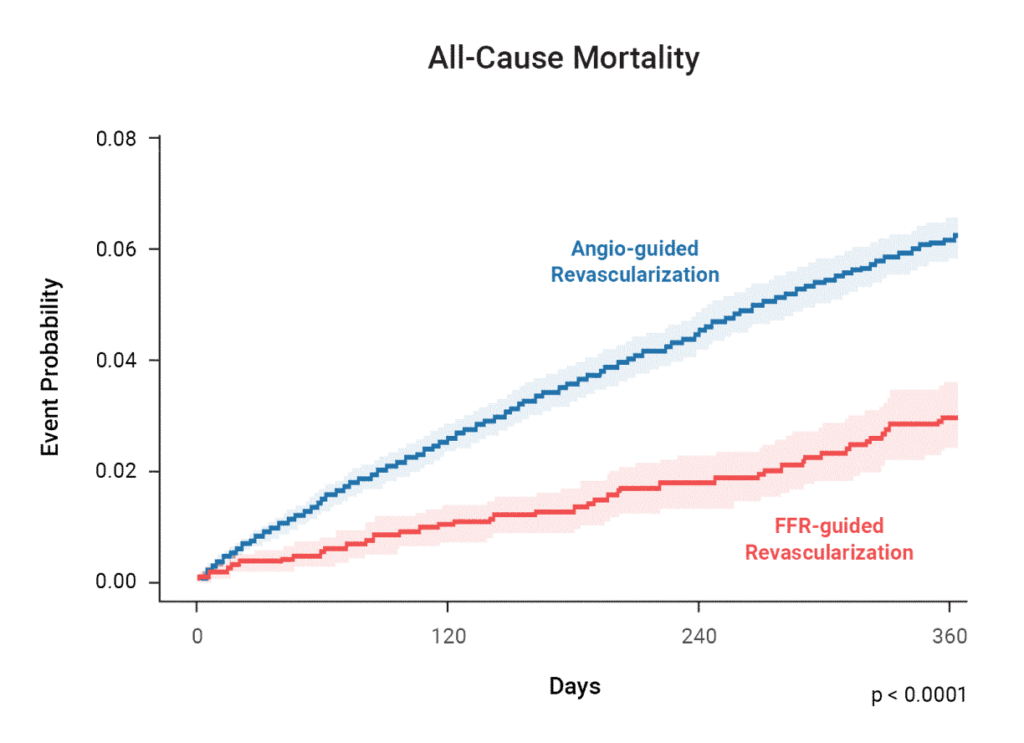
Adding physiologic insight to anatomy informs treatment and leads to better patient outcomes.8
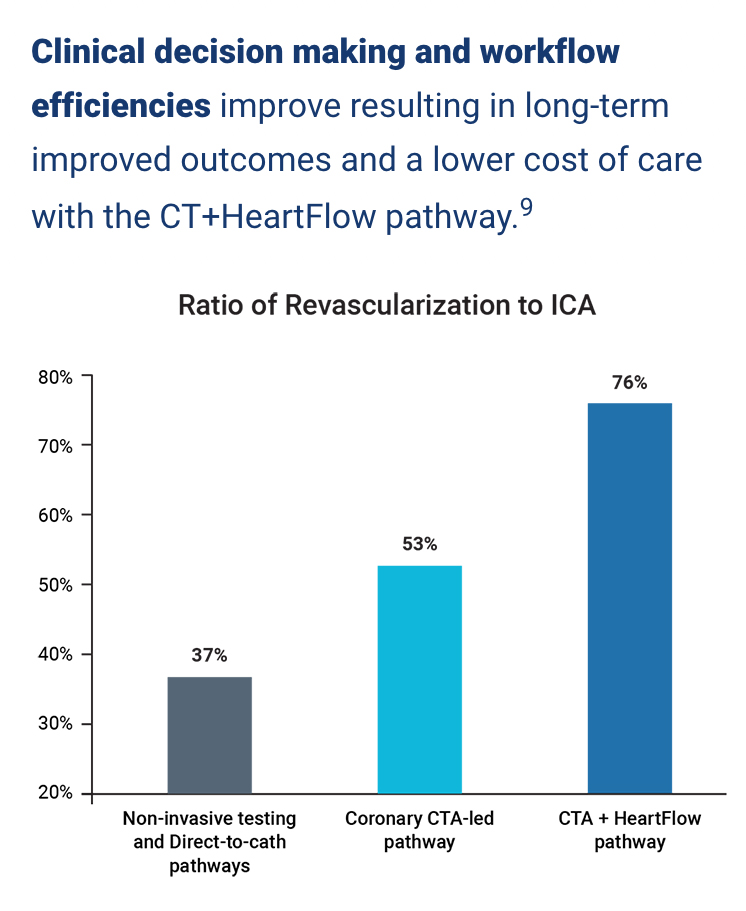
Clinical decision making and workflow efficiencies improve resulting in long-term improved outcomes and a lower cost of care with the CT+HeartFlow pathway.9
| SPECT | Stress Echo | Coronary CTA | HeartFlow Analysis | |
|---|---|---|---|---|
|
Common Questions |
 |
 |
 |
 |
|
Does my patient have CAD? |
X |
X |
X |
X |
|
Do the vessels have plaque? |
|
|
X |
X |
|
Where are the coronary artery specific stenoses? |
|
|
X |
X |
|
Is there possible ischemia? |
X |
|
X |
X |
|
What are the lesion-specific functional limitations? |
|
|
|
X |
|
Which vessels may benefit from PCI/CABG/OMT? |
|
|
|
X |
|
Is prognostic information provided? |
X |
X |
X |
X |
|
Diagnostic Performance* |
Sensitivity: 0.42 Specificity: 0.97 AUC: 0.792 |
Sensitivity: 0.77 Specificity: 0.75 AUC: 0.7010 |
Sensitivity: 0.68 Specificity: 0.83 AUC: 0.832 |
Sensitivity: 0.90 Specificity: 0.86 AUC: 0.942 |
|
Disadvantages2, 10-14 |
Low sensitivity; high rate of false negatives; higher radiation exposure; lacks anatomic data
|
Often requires additional testing; lacks anatomic data
|
High sensitivity can lead to overutilization of invasive testing when not paired with functional information
|
Requires CCTA; Currently not as well known as other tests
|
|
Advantages2, 10-14 |
Accessible; high specificity; standard of care
|
Accessible; no radiation
|
Better long-term outcomes than usual care testing; lower radiation; provides anatomic data
|
More accurate than other non-invasive tests; provides anatomic and functional information; lower radiation; single patient visit
|
* Diagnostic performance of SPECT, CCTA and FFRCT evaluated in a head-to-head comparison for the identification of ischemia.
| SPECT | Stress Echo | Coronary CTA | HeartFlow Analysis |
| HeartFlow Analysis | |
|---|---|
|
Common Questions |
 |
| Stress Echo | |
|---|---|
|
Common Questions |
 |
| Coronary CTA | |
|---|---|
|
Common Questions |
 |
| SPECT | |
|---|---|
|
Common Questions |
 |
|
Does my patient have CAD? |
X |
|||
|
Do the vessels have plaque? |
|
|||
|
Where are the coronary artery specific stenoses? |
|
|||
|
Is there possible ischemia? |
X |
|||
|
What are the lesion-specific functional limitations? |
|
|||
|
Which vessels may benefit from PCI/CABG/OMT? |
|
|||
|
Is prognostic information provided? |
X |
|
Does my patient have CAD? |
X |
|||
|
Do the vessels have plaque? |
|
|||
|
Where are the coronary artery specific stenoses? |
|
|||
|
Is there possible ischemia? |
X |
|||
|
What are the lesion-specific functional limitations? |
|
|||
|
Which vessels may benefit from PCI/CABG/OMT? |
|
|||
|
Is prognostic information provided? |
X |
|
Does my patient have CAD? |
X |
|||
|
Do the vessels have plaque? |
X |
|||
|
Where are the coronary artery specific stenoses? |
X |
|||
|
Is there possible ischemia? |
|
|||
|
What are the lesion-specific functional limitations? |
|
|||
|
Which vessels may benefit from PCI/CABG/OMT? |
|
|||
|
Is prognostic information provided? |
X |
|
Does my patient have CAD? |
X |
|||
|
Do the vessels have plaque? |
X |
|||
|
Where are the coronary artery specific stenoses? |
X |
|||
|
Is there possible ischemia? |
X |
|||
|
What are the lesion-specific functional limitations? |
X |
|||
|
Which vessels may benefit from PCI/CABG/OMT? |
X |
|||
|
Is prognostic information provided? |
X |
|
Diagnostic Performance* |
Sensitivity: 0.42 Specificity: 0.97 AUC: 0.792 |
|
Disadvantages2, 10-14 |
Low sensitivity; high rate of false negatives; higher radiation exposure; lacks anatomic data
|
|
Advantages2, 10-14 |
Accessible; high specificity; standard of care
|
|
Diagnostic Performance* |
Sensitivity: 0.77 Specificity: 0.75 AUC: 0.7010 |
|
Disadvantages2, 10-14 |
Often requires additional testing; lacks anatomic data
|
|
Advantages2, 10-14 |
Accessible; no radiation
|
|
Diagnostic Performance* |
Sensitivity: 0.68 Specificity: 0.83 AUC: 0.832 |
|
Disadvantages2, 10-14 |
High sensitivity can lead to overutilization of invasive testing when not paired with functional information
|
|
Advantages2, 10-14 |
Better long-term outcomes than usual care testing; lower radiation; provides anatomic data
|
|
Diagnostic Performance* |
Sensitivity: 0.90 Specificity: 0.86 AUC: 0.942 |
|
Disadvantages2, 10-14 |
Requires CCTA; Currently not as well known as other tests
|
|
Advantages2, 10-14 |
More accurate than other non-invasive tests; provides anatomic and functional information; lower radiation; single patient visit
|
Click to expand
Click to collapse
Click to expand
* Diagnostic performance of SPECT, CCTA and FFRCT evaluated in a head-to-head comparison for the identification of ischemia.
Click to collapse
Are you ready to make the change? Whether you are an avid user of stress tests and curious to learn more about the benefits of the CT + HeartFlow pathway, are looking to build a CT program and need help figuring out where to start or have a growing program but need to better understand how physiology fits in, contact our team. We’re ready to help. In the meantime, review some of the helpful resources below to learn more.
* Required fields
REFERENCES
The information provided by the HeartFlow Analysis is intended to be used in conjunction with the patient’s clinical history, symptoms, and other diagnostic tests, as well as the clinician’s professional judgement. The HeartFlow Analysis may not be appropriate for all patients. See indications for use for more information. The HeartFlow Analysis, featuring the FFRCT Analysis, RoadMapTM Analysis, Plaque Analysis, and HeartFlow Planner, has received FDA Clearance in the United States of America. The FFRCT Analysis and HeartFlow Planner are CE Marked in Europe and the United Kingdom and approved in Japan and Canada. The HeartFlow Analysis, featuring FFRCT Analysis, RoadMapTM Analysis, Plaque Analysis, and HeartFlow Planner, is commercially available in the United States. The FFRCT Analysis and HeartFlow Planner are commercially available in the United Kingdom. The FFRCT Analysis is also commercially available in Europe, Japan, and Canada.
© 2024 HeartFlow, Inc. | HeartFlow and the HeartFlow logo are registered trademarks of HeartFlow, Inc. Additionally, RoadMap is claimed as a trademark of HeartFlow, Inc. www.heartflow.com | 331 E Evelyn Ave, Mountain View, CA 94041
*Required fields
If you would like to request to have the HeartFlow Analysis available at a location near you, please submit your information below with details of the institution. We will share this information with the institution, but it will not guarantee HeartFlow will become available.
*Required fields
オンライン提出フォームから研究助成金を申請してください。
HeartFlow FFRCT 分析は、有資格の臨床医による臨床的に安定した症状のある冠状動脈疾患患者への使用を目的とした個別化された心臓検査です。 HeartFlow Analysis によって提供される情報は、資格のある臨床医が患者の病歴、症状、その他の診断検査、および臨床医の専門的判断と組み合わせて使用することを目的としています。
ハートフロー分析に関する追加の適応情報については、次のサイトをご覧ください。www.heartflow.com/indications.
さらに質問がある場合は、このメッセージを閉じてフォームに記入するか、サポート チームにお電話ください。: 877.478.3569.
The HeartFlow FFRCT Analysis is a personalized cardiac test indicated for use in clinically stable symptomatic patients with coronary artery disease by qualified clinicians. The information provided by the HeartFlow Analysis is intended to be used by qualified clinicians in conjunction with the patient’s history, symptoms, and other diagnostic tests, as well as the clinician’s professional judgement.
For additional indication information about the HeartFlow Analysis, please visit www.heartflow.com/indications.
If you have additional questions, close out of this message to complete our form or call our support team: 877.478.3569.Please use our online submission form on the Clinical Research Page to apply for research grants.
Thank you for your interest!

Executive Vice President and Chief Medical Officer
Campbell brings a wealth of experience to HeartFlow, where he serves as the Chief Medical Officer. Prior to joining HeartFlow, he was the Chief Scientific Officer and Global Head of Research and Development at Cordis Corporation, Johnson & Johnson, where he was responsible for leading investments and research in cardiovascular devices. Prior to Cordis, he was Associate Professor of Medicine at Harvard Medical School and the Harvard-M.I.T. Division of Health Sciences and Technology, and Director of the Cardiac Catheterization and Experimental Cardiovascular Interventional Laboratories at Brigham and Women’s Hospital. He served as Principal Investigator for numerous interventional cardiology device, diagnostic, and pharmacology trials, is the author of numerous journal articles, chapters, and books in the area of coronary artery and other cardiovascular diseases, and was the recipient of research grant awards from the NIH and AHA.
He received his A.B. from Harvard College and his M.D. from Harvard Medical School.