Precision over Intuition: CT-Guided PCI Spells the End of Flying Blind in the Cath Lab
For decades, interventional cardiology has relied on a reactive workflow. Traditionally, we would enter the lab, perform a coronary angiography, and determine our strategy on the fly. In many ways, we have been flying blind—relying on 2D snapshots to navigate complex, 3D anatomy.
But the shift toward CT-guided PCI is fundamentally changing the game. We are moving away from figuring it out as we go and toward entering the cath lab with a comprehensive, data-driven procedural roadmap for navigating the procedure. By shifting our decision-making to the pre-procedural phase, we address several critical gaps that traditional PCI cannot reach.
Improving Cath Lab Efficiency: Eliminating the “Supply Closet Shuffle”
Operational efficiency is about more than just Wheels Out to Wheels In time. When an operator knows the optimal guiding catheter and stent dimensions before the patient even enters the room, the entire environment changes. We eliminate the “supply closet shuffle” where staff are often running for different tools mid-procedure. This won’t just save time; it will likely increase the capacity of the entire cardiovascular service line.
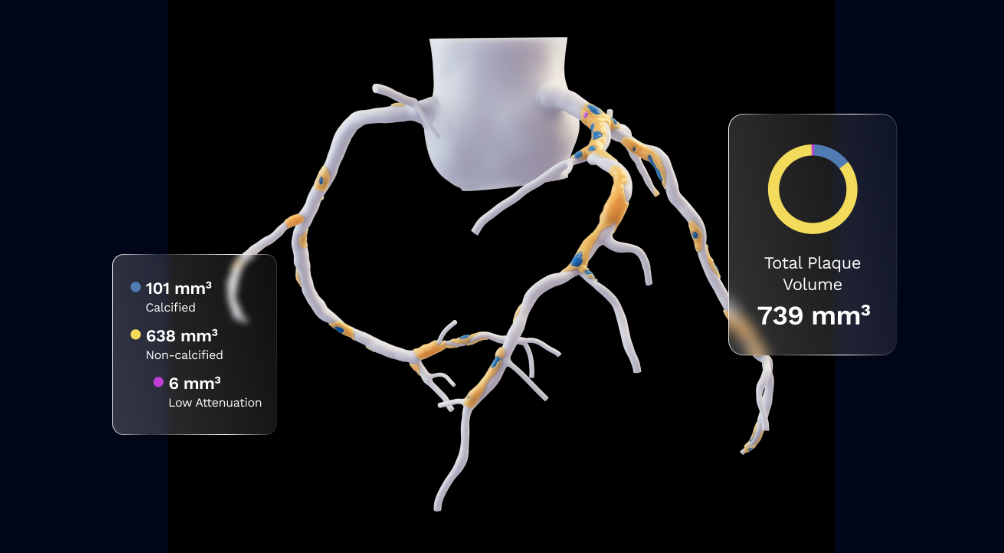
Identifying Plaque Morphology and Calcification Before the Procedure
A standard angiogram often fails to reveal the true nature of a lesion. By using CT-guided analysis, we can identify localized plaque characteristics—like extreme eccentricity or heavy calcification—long before the first wire touches the patient. This visibility enables us to decide in advance if we need specialized pre-treatments like Shockwave (IVL) for plaque modification or atherectomy for calcium modification, ensuring we optimally deploy every stent the first time.
Using FFRCT for Targeted Revascularization and Flow Improvement
Choosing target lesions based on stenosis and plaque alone leads to missed opportunities to improve PCI outcomes. Instead, having an immediate line of sight to specific locations of flow impairment through FFRCT virtual pullbacks, co-registered to coronary anatomy in a lesion-specific manner, can help ensure an optimal revascularization strategy.
How Procedural Efficiency Enhances Patient Safety and Access
We often think of safety on a case-by-case basis, but we must also look at it through the lens of patient access. A streamlined, efficient cath lab means more patients can be treated. When we optimize our throughput, we ensure that elective patients aren’t waiting at home through a weekend because the lab is booked. Greater procedural efficiency is designed to help reduce unnecessary radiation exposure and contrast use—further enhancing patient safety during each procedure. In a field where time is muscle, getting a patient on the table sooner is one of the most impactful safety measures we have.
Quantifying Myocardial Risk: Data-Driven Decision Making for PCI
Finally, this CT-guided PCI allows for a more sophisticated risk-benefit assessment. By understanding exactly what percentage of the myocardium a vessel supplies, we can move beyond simply looking at the complexity of a lesion and focus on its functional significance. It allows us to ask the most important question: Is the risk of this intervention justified by the amount of heart muscle at stake? This level of insight ensures we’re prioritizing the procedures that will have the greatest impact on a patient’s long-term health.
I believe CT-guided PCI is quickly moving from a nice-to-have to the standard of care. I anticipate that it will be one of the most precise, non-invasive ways to optimize outcomes before the intervention even begins. Once an operator experiences the confidence of having a pre-defined map and the ability to act as an architect rather than an explorer, they simply won’t want to go back to flying blind.
See CAD. Manage for life.