A Unified Approach to Coronary Risk: Combining FFRct with Plaque Analysis
In my practice, the use of FFRCT technology has become table stakes. It provides the functional information we need to understand a lesion’s significance right at our fingertips, and it’s now a foundational part of our clinical guidelines. However, as we look at the overlap between physiology and disease, it’s clear that functional significance is only one piece of a much larger puzzle. To truly understand a patient’s risk, we have to look beyond the individual lesion and at the coronary tree as a whole.
Moving Beyond Stenosis Alone
While we’ve become very comfortable at identifying functional stenosis, it’s important to consider: what are we missing when we look at flow alone? I’ve cared for many patients who present with symptoms but return a non-significant FFRCT. In a traditional setting—especially with a standard coronary angiogram—those patients might be told they are fine. They might stay on a standard statin dose and be sent on their way because, realistically, no one is going to IVUS every vessel in that person’s heart. You aren’t going to check the right, the LAD, and the circumflex in every patient with a non-significant 50% lesion.
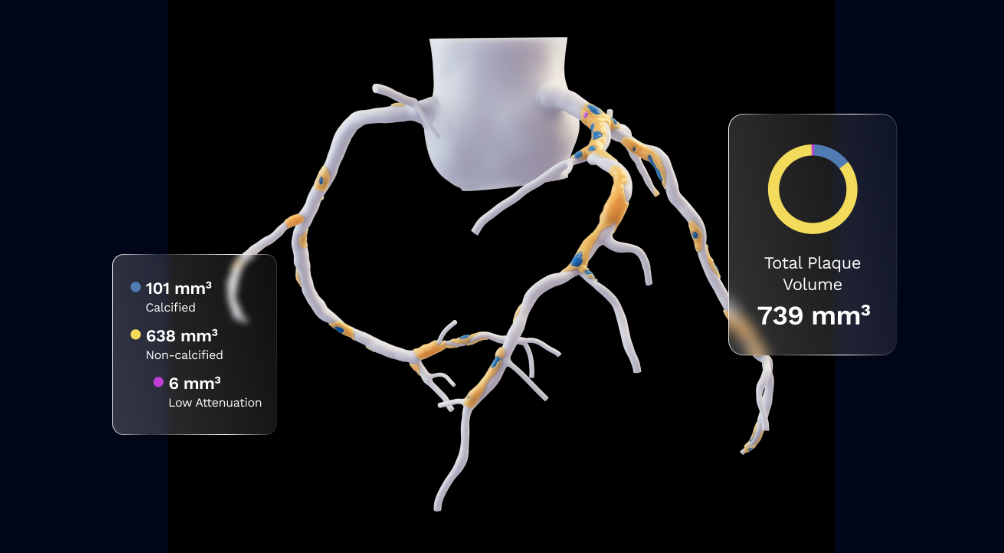
However, when you have plaque data available, the conversation changes. As we saw in the SCOT-HEART subgroup analysis, a total plaque volume greater than 238.5 mm3 is a very strong, independent predictor of myocardial infarction.1 Even if a lesion doesn’t have functional significance today, if that volume is 700, or if we see a high percentage of non-calcified plaque, we know we are looking at a vulnerable patient who likely needs more intensive medical management intervention.
Personalizing the Plan to Stabilize Plaque
Having both FFRCT and Plaque Analysis at our disposal gives us precise, individualized information about a patient’s prognosis. We are no longer just guessing at risk; we are looking at the actual characteristics of the disease. Trials like EVAPORATE and PACMAN-AMI have been landmark moments for us because they proved that we can actually modulate these plaque characteristics. We can stabilize vulnerable, non-calcified plaque and mitigate risk through intensive medical management. Importantly, plaque assessment allows us to understand not only the composition of the functionally significant lesion, but also the patient’s overall plaque burden and the presence of other high-risk lesions—giving us a more complete picture of risk.
The Advantage Outside the Exam Room
Outside of the exam room, this combined approach has become an essential part of my toolkit for navigating the administrative complexities of modern care. While securing coverage is never a guarantee, using the published plaque staging framework from the DECIDE registry provides a much-needed layer of scientific validity during the prior authorization process. When we can point to data showing extensive or severe plaque, we’re better able to provide the clinical evidence that often helps bridge the gap for LDL-lowering therapies.
The Future of Comprehensive Care
By integrating FFRCT and Plaque Analysis, we move from the narrow focus of identifying blockages to the broader goal of managing a patient’s long-term cardiovascular health. FFRCT technology gives us the functional answers we need for the lesion in front of us today, but Plaque Analysis provides a window into that patient’s future risk. We have a remarkable opportunity to move from a reactive model to a truly proactive one. By leveraging both technologies, we ensure that no high-risk patient remains invisible, allowing us to provide the most precise, individualized care possible.
See CAD. Manage for life.