Closing the Diagnostic Gap in Women’s Heart Health
In cardiology, we’re increasingly recognizing that the traditional one-size-fits-all model for assessing coronary risk often misses the specific way cardiovascular disease manifests in women. For years, the symptoms and risk calculators we relied upon were built on data that didn’t fully account for how cardiovascular disease presents in women. Today, we have a remarkable opportunity to close that diagnostic gap, moving away from generalized assessments and toward a truly individualized understanding of risk.
Looking Beyond Traditional Risk Markers
A proactive evaluation for women should go beyond what we find on a standard lipid panel or a basic cholesterol screening. When I see a healthy, active woman in her 50s, I’m not just looking at her blood pressure or lab results—I’m also searching for the hidden drivers of disease that a blood test won’t reveal. We have to consider a clinical history that may be left out of the conversation: Was there a history of preeclampsia? Did she experience premature menopause? Going through menopause before age 40, for example, changes the vascular environment significantly. When we combine these biological milestones with the fact that women are more likely to have inflammatory risk enhancers like rheumatoid arthritis or lupus, we realize that a woman’s actual risk is often much higher than what a standard clinical assessment might indicate. Our goal is to make that risk visible long before it leads to a cardiac event.
Understanding Non-Obstructive Coronary Disease
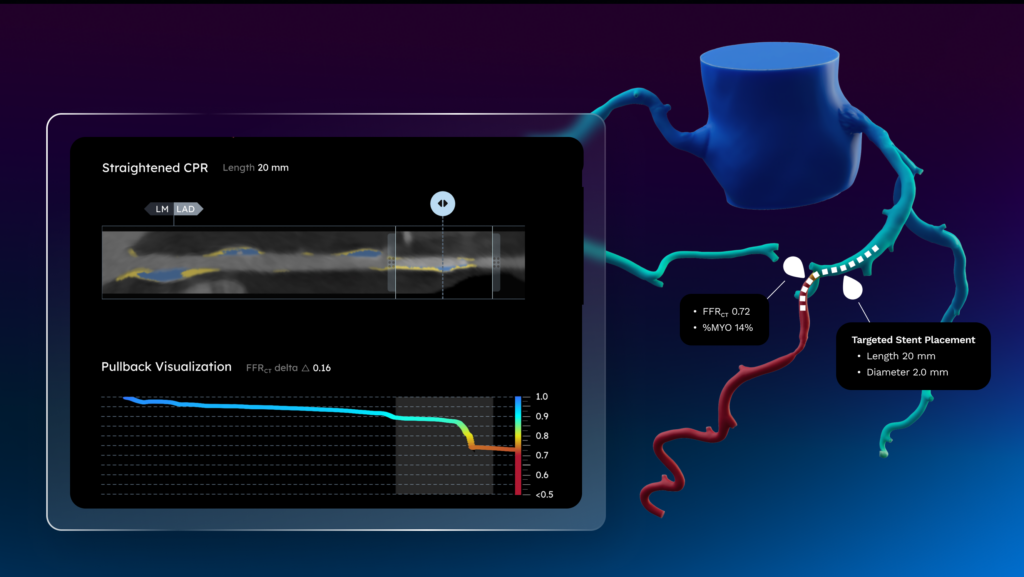
One of the nuances of treating women is the high prevalence of non-obstructive disease, or Angina with Non-Obstructive Coronary Arteries (ANOCA), which accounts for a significant portion of female cardiac symptoms. Because these cases don’t always present as a single, major blockage, they can be difficult to diagnose with traditional tests. This is where the integration of FFRct and AI-enabled Plaque Analysis acts as a powerful equalizer. By utilizing coronary CT imaging, we can exclude dangerous obstructive disease without an invasive procedure, while simultaneously identifying the soft or non-calcified plaque that is more common in younger women. This non-calcified plaque often stays under the radar of a standard calcium score, but identifying it early gives us a 10-to-20-year head start on the effort to stabilize the disease and potentially mitigate future risk.
Turning Objective Data Into Actionable Prevention
The most rewarding part of using these tools is the ability to empower women with their own data. Standard guidelines can sometimes make it difficult to justify intensive primary prevention in younger women because their age and gender may suggest they are low risk. However, seeing their plaque visualized in a vivid, interactive 3D model can completely change that narrative. It provides the scientific validity needed to personalize a care plan today, rather than waiting for a crisis tomorrow. It also allows us to educate our patients about their specific morphology and implement therapies that can prevent that plaque from becoming obstructive down the line.
The Shift Toward High-Value Care
Ultimately, the future of women’s cardiac care lies in high-value diagnostics. We know that 80% of coronary disease is preventable, but that prevention starts with an accurate estimate of risk. By leveraging FFRct and comprehensive plaque quantification, we have the opportunity to move past the limitations of the past and provide the women we treat with a clearer, more precise roadmap for managing their long-term heart health.
See CAD. Manage for life.