Helping physicians get the right patient,
the right care at the right time.
This image is not an accurate representation of the HeartFlow product
The PRECISE Trial
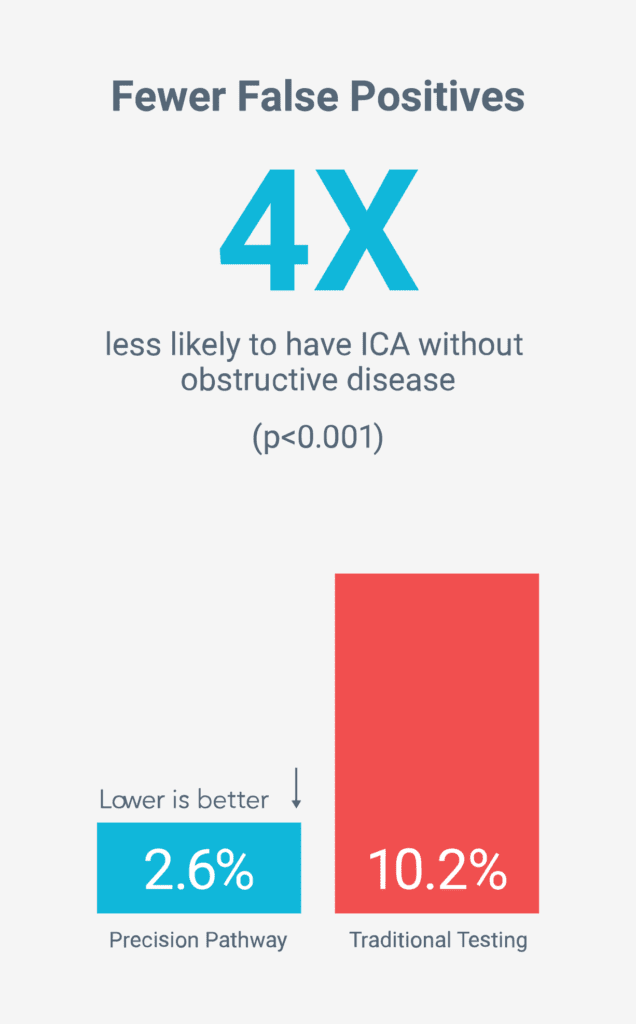
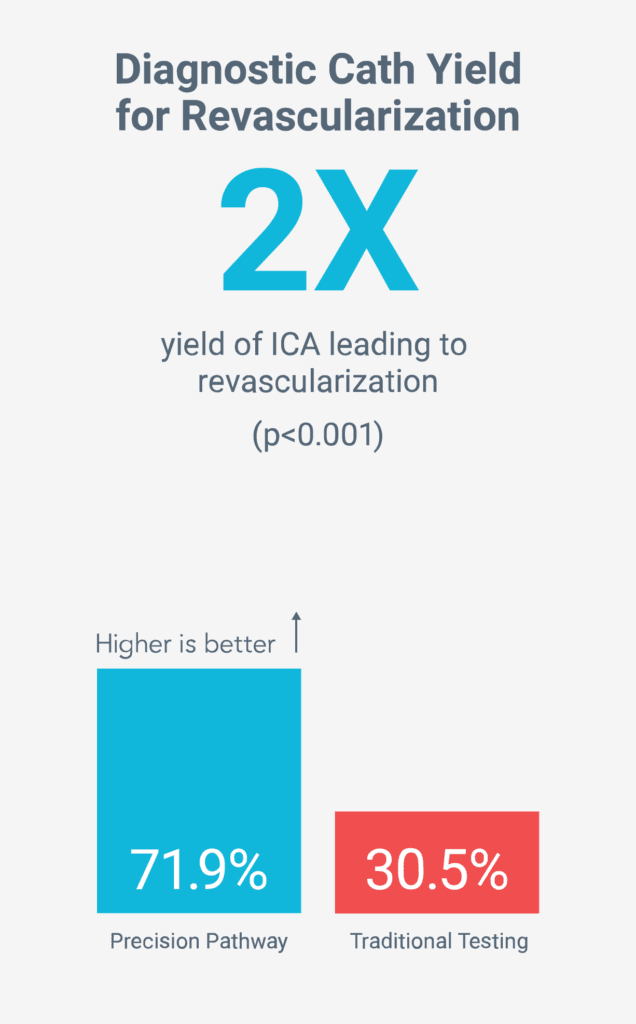
It’s confirmed. The Precision Pathway recognized in the AHA/ACC guidelines — centered around Coronary CTA+FFRCT — is superior to Traditional Testing, which prioritizes functional (stress) testing and Invasive Coronary Angiography (ICA).1
Physician Perspectives on the PRECISE Trial
The PRECISE Trial – A conversation with Dr. James Udelson, Tufts Medical Center
KOLs Agree! PRECISE supports Chest Pain Guidelines, CCTA+FFRCT Pathway good for patient care, cath lab efficiency
PRECISE 1 Year Results Quick Summary with Pam Douglas
A closer look at the PRECISE Trial
Webinar: This panel of leading experts discusses insights from the PRECISE Trial 1-Year data, how the findings relate to the 2021 AHA/ACC Chest Pain Guidelines, and what the data tell us about different strategies for the evaluation and diagnosis of coronary artery disease. Featuring Dr. Pamela S. Douglas, Dr. Maros Ferencik, and Dr. Gregg W. Stone
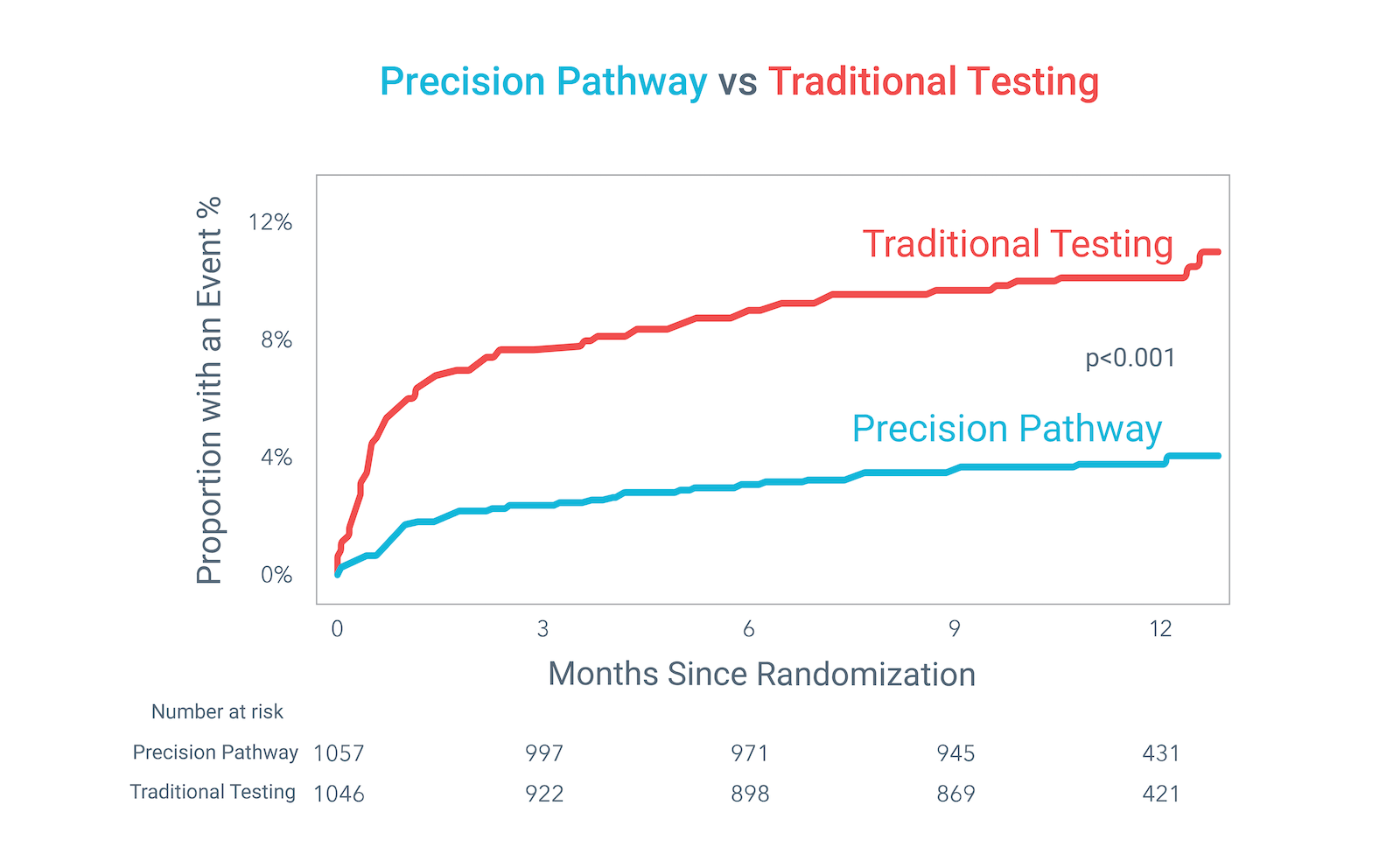
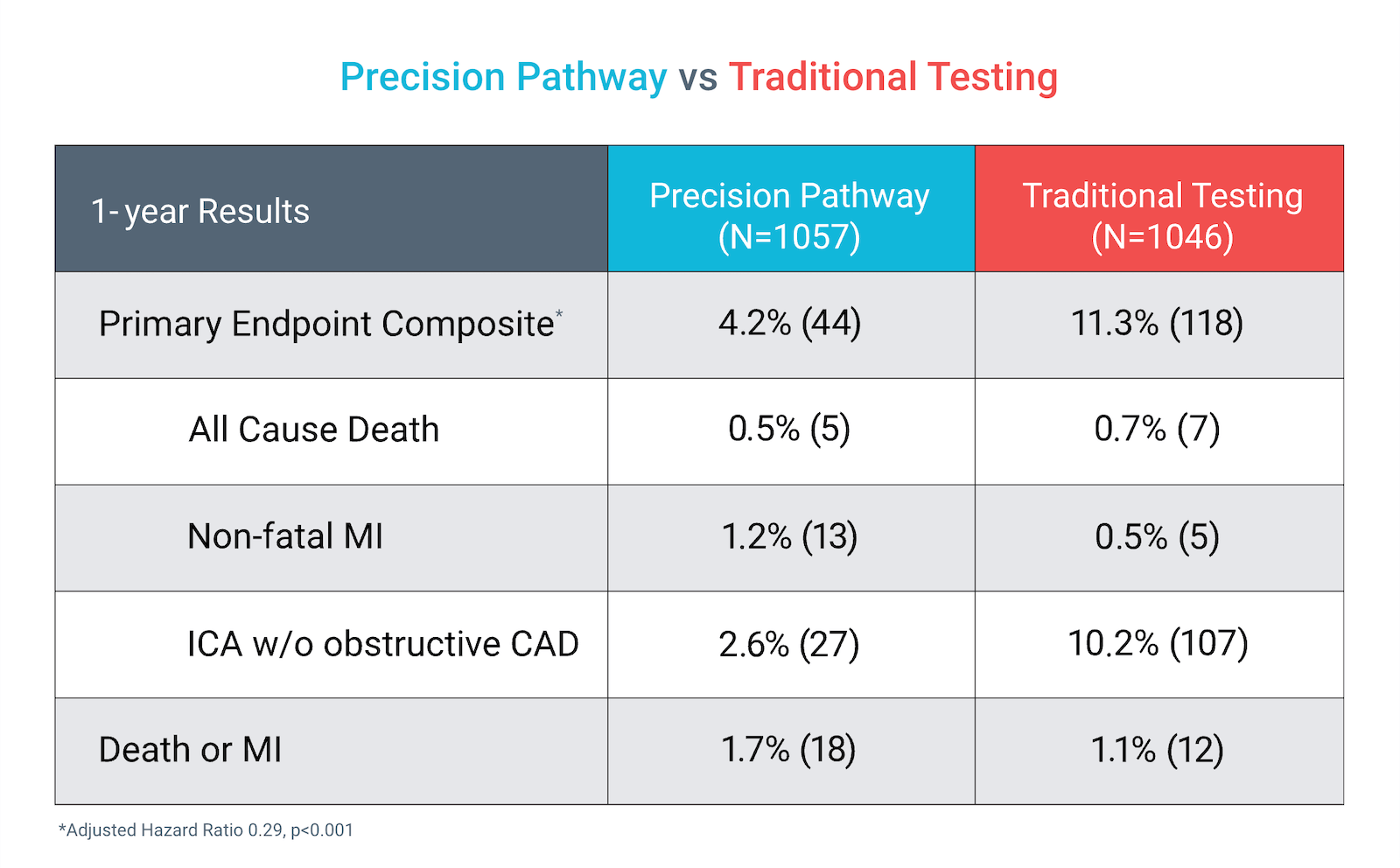
The Precision Pathway, centered around CCTA+FFRCT, achieved its primary endpoint by significantly reducing the composite of all-cause death, nonfatal MI, or catheterization without obstructive disease relative to Traditional Testing at 1 year.
KM CHART
COMPOSITE
KM CHART
COMPOSITE
KM CHART
COMPOSITE
KM CHART
COMPOSITE
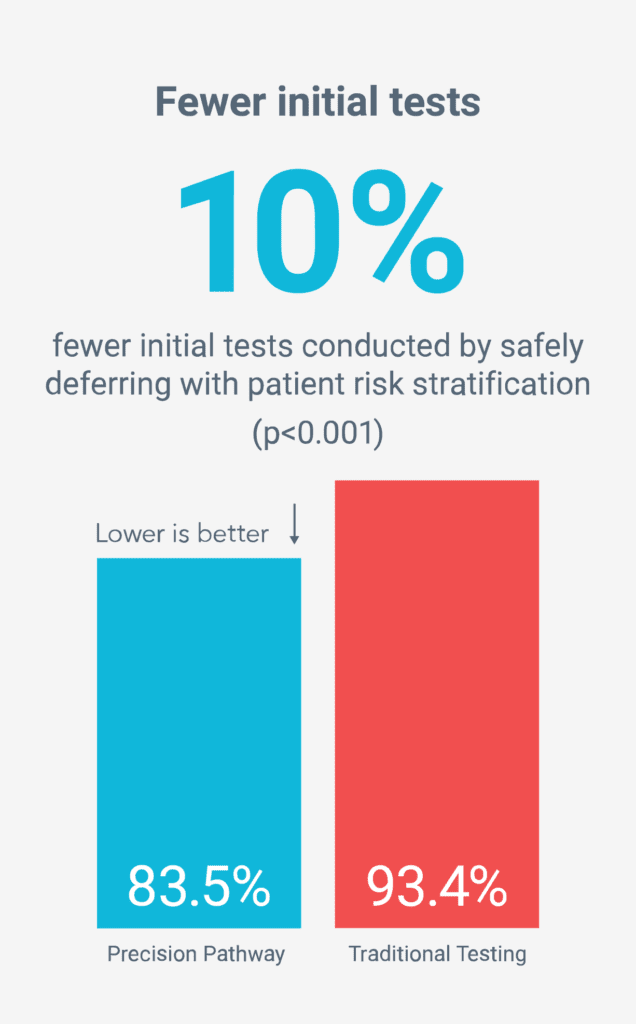
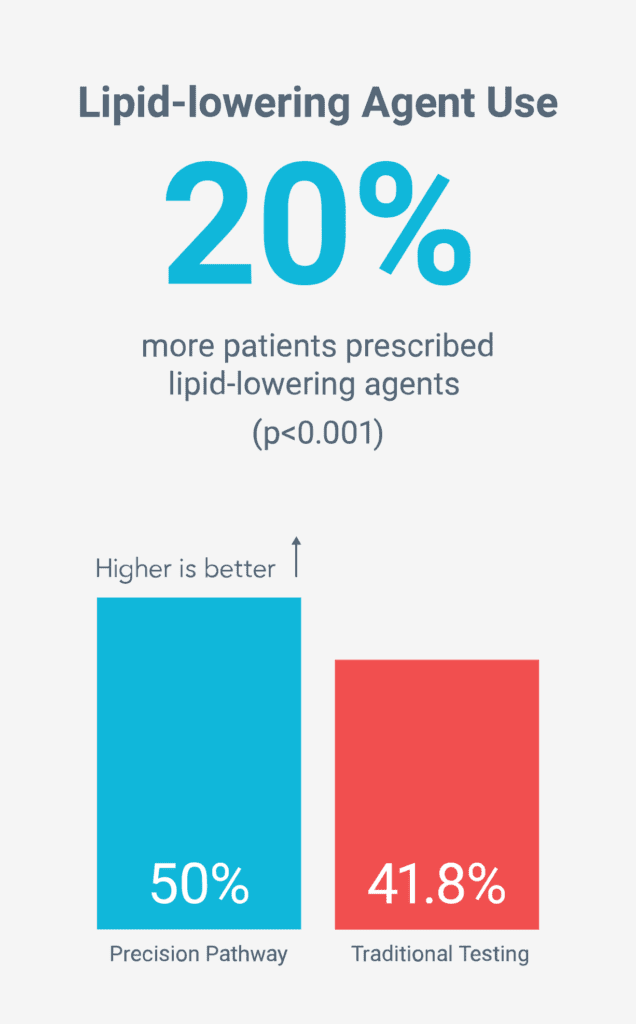
Key Findings
Precision Pathway compared to Traditional Testing:
65
Global Sites
2,103
Patients
Adjudicated
Core Lab, CEC2
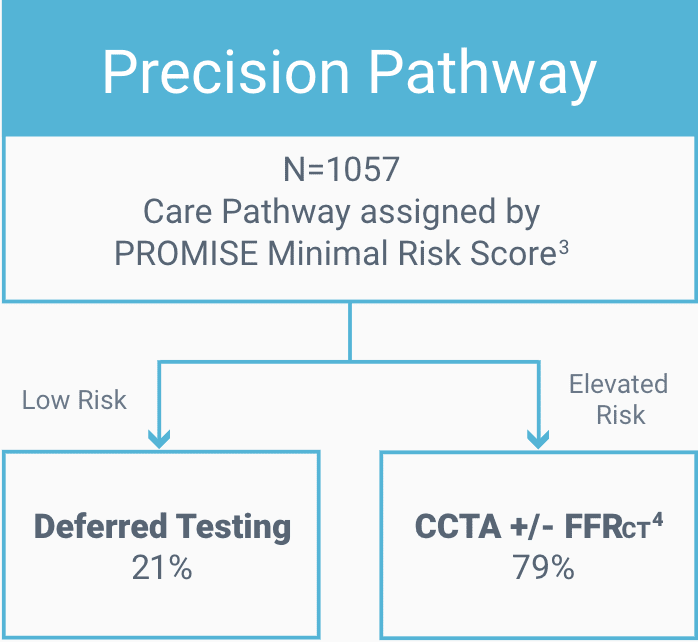
Precision Pathway
Risk scoring to defer testing for low-risk patients.3
CCTA with selective FFRCT4 for elevated risk patients.
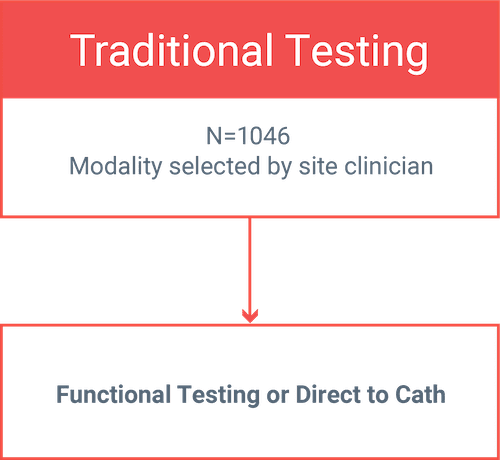
Traditional Testing
Functional testing (stress nuclear and stress echo) and Invasive Coronary Angiography (ICA).
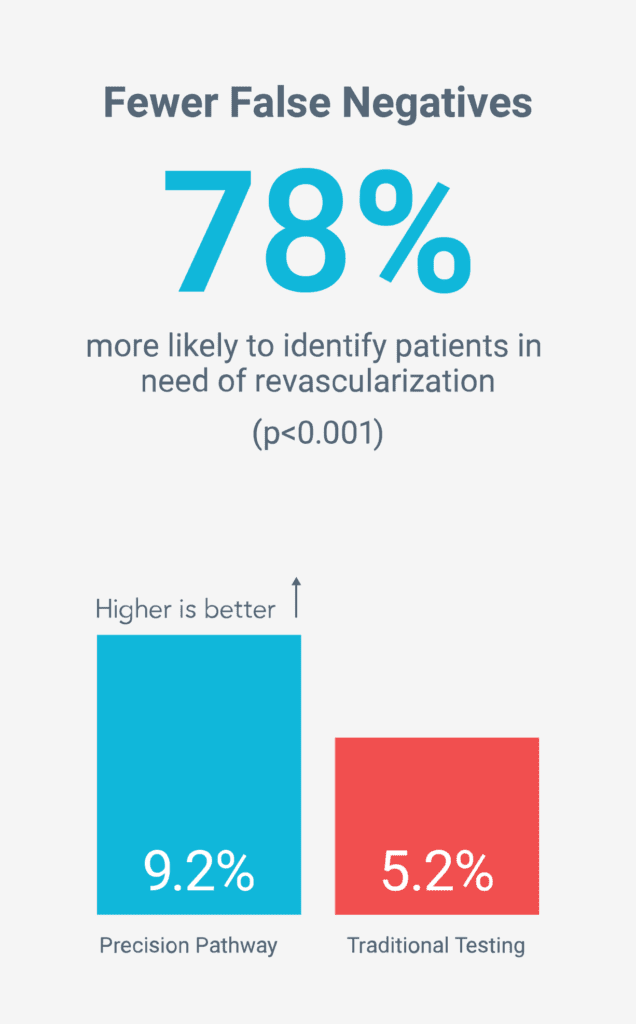
More accurate non-invasive diagnosis
Fewer unnecessary tests
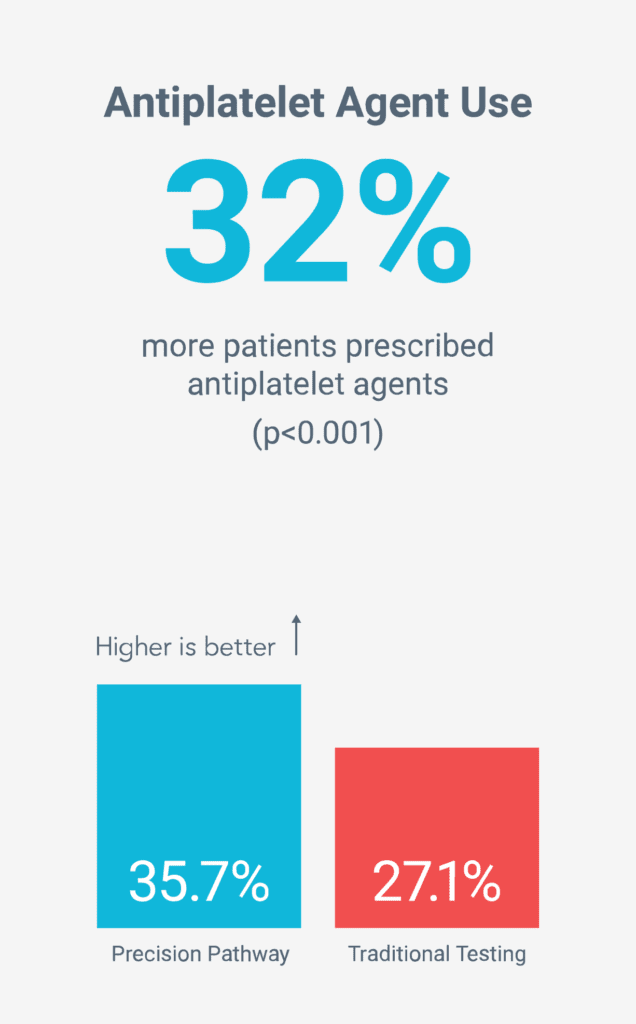
Reduced long-term risk by increasing preventive therapies5
Patients with non-acute chest pain or the equivalent requiring testing for suspected CAD.
No history of Obstructive CAD or CAD testing < 1 year: N=2103
Randomized into one of two pathways. Randomization stratified by site, PROMISE Minimal Risk Score (Low Risk vs. Elevated Risk), and intended first test (if randomized to Traditional Testing).
All subsequent care and testing decisions made by site clinician. Guideline-directed medical management recommended for all.
Douglas, et al. Comparison of an Initial Risk-Based Testing Strategy vs Usual Testing in Stable Symptomatic Patients With Suspected Coronary Artery Disease. JAMA Cardiol. 2023.
Clinical Events Committee (CEC)
Patient risk was determined using the PROMISE Minimal Risk Score. PROMISE variables include: age, sex, ethnicity, smoking history, diabetes mellitus, dyslipidemia, family history of premature coronary artery disease, hypertension, symptoms related to stress and high-density lipoprotein (HDL) concentration.
For stenoses 30-90%
Joshi, et al. JAMA 2021.
Contact Us
*Required fields
Request the HeartFlow Analysis Near You
If you would like to request to have the HeartFlow Analysis available at a location near you, please submit your information below with details of the institution. We will share this information with the institution, but it will not guarantee HeartFlow will become available.
*Required fields
残念ながら、GDPR 規制により、この Web フォームを通じて求人への応募やキャリアに関する問い合わせを受け付けることはできません。弊社を通じてお申込みください 採用ページ. ご関心をお寄せいただきありがとうございます!
The HeartFlow FFRCT Analysis is a personalized cardiac test indicated for use in clinically stable symptomatic patients with coronary artery disease by qualified clinicians. The information provided by the HeartFlow Analysis is intended to be used by qualified clinicians in conjunction with the patient’s history, symptoms, and other diagnostic tests, as well as the clinician’s professional judgement.
If you have additional questions, close out of this message to complete our form or call our support team: 877.478.3569.
Please use our online submission form on the Clinical Research Page to apply for research grants.
Thank you for your interest!
Unfortunately, we cannot take job applications or career inquiries through this web form due to GDPR regulations. Please apply through our Careers Page. Thank you for your interest!
Campbell Rogers, M.D., F.A.C.C.
Executive Vice President and Chief Medical Officer
Campbell brings a wealth of experience to HeartFlow, where he serves as the Chief Medical Officer. Prior to joining HeartFlow, he was the Chief Scientific Officer and Global Head of Research and Development at Cordis Corporation, Johnson & Johnson, where he was responsible for leading investments and research in cardiovascular devices. Prior to Cordis, he was Associate Professor of Medicine at Harvard Medical School and the Harvard-M.I.T. Division of Health Sciences and Technology, and Director of the Cardiac Catheterization and Experimental Cardiovascular Interventional Laboratories at Brigham and Women’s Hospital. He served as Principal Investigator for numerous interventional cardiology device, diagnostic, and pharmacology trials, is the author of numerous journal articles, chapters, and books in the area of coronary artery and other cardiovascular diseases, and was the recipient of research grant awards from the NIH and AHA.
He received his A.B. from Harvard College and his M.D. from Harvard Medical School.